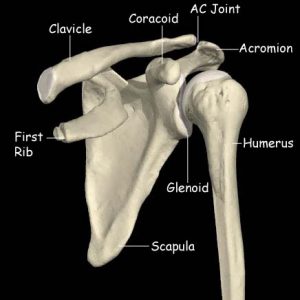
The clavicle or collar bone connects the sternum (breast bone) to the shoulder. It is a slim bone and is vulnerable to fracture
What Causes it?
Nearly all clavicle fractures are as a result of a fall or a direct blow. What are the symptoms?Pain at the site of the fracture
Visible deformity with the end of the bone often being close to the skin Rarely, numbness and tingling in the handHow is the diagnosis made?
The doctor will listen to the description of the symptoms and will examine the shoulder. Plain X-rays are usually sufficient to make the diagnosis. If the ere any concern about the nerves or the fracture is particularly complex then MRI and CT scans may also be undertaken.

What is the initial treatment?
The vast majority of clavicle fractures heal with non-operative treatment. Traditionally the arm is placed in a sling but we prefer a clavicle brace which is more comfortable and allows the hands to be free.
 Typical clavicle brace, these are readily available quite cheaply on the internet
The progress of the healing is monitored. X-rays will be taken (typically 6 weeks after the initial injury). Further decisions can then be made.
Early surgical treatment is more likely in the following cases:If the bone ends are far apart on the x-rays
If there is any concern about the nerves
If the occupation includes wearing heavy rucksacks or body armour regularly
If there are other injuries and fixing the clavicle would help with nursing care
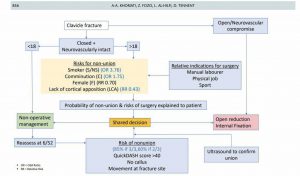
Algorithm for clavicle fracture management
Typical clavicle brace, these are readily available quite cheaply on the internet
The progress of the healing is monitored. X-rays will be taken (typically 6 weeks after the initial injury). Further decisions can then be made.
Early surgical treatment is more likely in the following cases:If the bone ends are far apart on the x-rays
If there is any concern about the nerves
If the occupation includes wearing heavy rucksacks or body armour regularly
If there are other injuries and fixing the clavicle would help with nursing care
Algorithm for clavicle fracture management
If initial treatment doesn’t work, what’s next?
If the clavicle is predicted not to heal (typically at 6 weeks) or has not healed (usually after 3 months) AND the patient has symptoms then operative fixation of the clavicle may be appropriate.
Anaesthetic
General Anaesthetic with an interscalene block (You will be fully asleep and a local anaesthetic injection into the side of the neck will numb the nerves to the shoulder for post-operative pain relief)
Incision
An 8cm incision will be made just below and along the clavicle
clavicle incision
Procedure
The fracture will be prepared and a titanium plate with screws will be used to hold the fracture together while it heals.. The tissues will be sewn back to their original positions. We typically use the Acumed plating system

Acumed clavicle plate
Pain relief
The anaesthetist will discuss a nerve block which will be administered after you are asleep, this means that you will wake up with no pain in the shoulder but the arm will feel numb for up to 12 hours. You will be prescribed painkillers to start taking when you get home and we encourage you to take these regularly for at least the first few days. There will be some discomfort but this settles quite rapidly and ice packs can be used in addition if you wish.
Wound Closure
A single long dissolving stitch under the skin and paper stitches over the top will be used to close the wound. These stitches do not need to be removed
Dressings
A Tegaderm dressing will be placed over the top of the paper stitches.
Surgical Risks
Every operation has a degree of risk. It is important that you are aware of these risks before you agree to proceed with your operation. If you decide not to proceed with surgery there is a possibility that the symptoms will settle on their own but they may continue and they may get worse. You will not damage the shoulder if you decide not to proceed with surgery.
The most common or significant risks are outlined below. A risk of 0.1% means that 1 in 1000 people will suffer the complication
- Failure of the procedure to relieve symptoms: 5%
- Superficial Infection (requiring antibiotics): 1%
- Deep Infection (requiring further surgery): <1%
- Need to remove the plate and screws (after a minimum of 1 year) <10%
- PE (Pulmonary Embolus) (Blood clot in the lung): 0.13% – Blood thinning medication is required for several months. Can rarely result in death.
- DVT (Deep Vein Thrombosis) (Blood clot in the leg): 0.14% – Blood thinning medication is required for several months. Can lead to PE
- Nerve Injury: 0.01% – Usually temporary. Can cause weakness around the shoulder with loss of function and rarely can be permanent.
- Heart attack: 0.02%
- To put these numbers in perspective The chance of:
- Getting three balls in the UK national lottery: 0.9%
- Needing emergency treatment in the next year after being injured by a can, bottle, or jar: 0.1%
- Death by an accident at home: 0.01%
- For a 50 year old man in good health the 5 year risk of dying is 0.8%
Rehabilitation after surgery
You will wake up with a sling on your arm and your arm may feel numb for the rest of the day. you can usually go home the same day.
Day 1:
- You may shower with the dressings on but do not immerse the wound in water for 2 weeks.
- Start gentle exercises to prevent elbow and wrist from becoming stiff.
Day 2 (approx):
- Start exercises for the shoulder
- External rotation (out to the side)
- no raising the arm to the front or the side beyond the horizontal
- sling when not doing exercises
- External Rotation to the limit set in the Operation Note
- Remove the dressings at 10-14 days.
- The paper stitches will peel off easily. No stitches need to be removed.
- You will be seen in clinic at 3 weeks where X-rays will be taken and plans for formal physiotherapy will be made.
Frequently asked questions
What happens if the clavicle doesn’t heal? Non-union (failing to heal) is not common. For many people there is no problem. They have no pain and can do all their activities. Do I have to have an operation if it doesn’t heal? You only need an operation if the clavicle is causing you any problems. Is there a downside to having the surgery when the clavicle hasn’t healed compared to immediately after injury? No. The surgery itself is basically the same and the recovery period is identical. The only downside is the time out from the original injury. All studies suggest that by 1 year after the injury everyone is the same regardless of which pathway they take. Do I have to have the plate and screws removed later? No. The metalwork can stay forever. It is only removed if it is irritating you (sometimes this happens in very slim people). There is a theoretical risk of further problems in people who play contact sports and you should discuss this if it applies to you.Return to work after surgery
This is very much dependent on the type of work that you do, whether you need to drive to get to work and the type of surgery that you have had done.
You, as the patient, have the best idea of the specific demands that are required of you to do your work safely and effectively.
Having an operation with an anaesthetic often takes more out of people than they would expect. Generally it is probably worth taking at least a week off from your regular work after having had any procedure.
You should discuss expected post-operative recovery and work with the surgeon before your operation.
Driving after surgery
To be able to drive safely you should be capable of actively moving your shoulder without assistance and without damaging the surgical repair. You should be able to react normally to avoid causing injury to yourself or others due to a lack of control.
Typically this is a MINIMUM eight weeks after surgery.
It is a UK requirement that, unless specific dispensation has been granted by the DVLA, a driver uses both arms to control the steering wheel.
It is the responsibility of the driver to ensure that they are in control of the vehicle at all times. They should be able to demonstrate this if stopped by the police.
It is not a requirement to notify the DVLA unless the medical conditions likely to affect safe driving persist for longer than three months after the date of the surgery.
Drivers must not drive under the influence of narcotic medications or within a minimum of 24 hours after an anaesthetic.
You are not allowed to drive one-handed and therefore cannot drive whilst you are in the sling.
There is no precise time after surgery when you can return to driving, it varies from person to person. However, the recommended amount of time that your arm should be in a sling following surgery is the MINIMUM time before considering a return to driving.
You can return to driving when you are capable of moving your shoulder without assistance and are capable of driving safely and reacting appropriately in an emergency situation.
Although it is not essential, it may be wise to discuss your return to driving with your car insurance company.
Sports after surgery
You can start simple cardio such as walking or using a static bicycle immediately following surgery as long as you are wearing your sling. Exercises which involve the shoulder cannot start until you have regained reasonable range. This is typically about eight weeks following surgery.